The case that landed on my desk
The case that landed on my desk seemed straightforward at first glance. A 26‑year‑old college graduate and former Marine had broken an emergency medical technician’s nose with a single punch after she responded to a late‑night call at his home. A few familiar scenarios came to mind: an alcohol‑fueled domestic dispute, a drug reaction, or a late‑breaking impulse‑control problem. Those are common enough, but you have to begin a case like this with an open mind.
In my line of work, claims of amnesia come up often and usually aren’t true. It can happen with alcoholic blackouts. People often think an “alcoholic blackout” means you suddenly lose consciousness. In reality, you can stay awake and engage in purposeful activity—talk, walk, drive—and the people around you may just think you’re drunk, not that part of your brain is offline. What’s actually happening is a form of anterograde amnesia, meaning your brain has temporarily stopped forming new memories, so the events never get recorded even though you were there for them. In my experience, though, it is very unusual for someone to carry out a complex, goal‑directed act like robbing a bank or committing a planned murder and then have a true, complete blackout for the entire event; those kinds of claims are far more likely to reflect exaggeration, avoidance, or simple wishful thinking than genuine memory loss.
I’ve had a version of this myself, not with alcohol but with propofol during surgery. I remember chatting with the nurse in the pre‑surgery bay, and my next clear memory is of sitting in a recliner while she helped me put my socks on. When my memory “came back online,” I was mid‑sentence, talking away with her as if the conversation had never paused. She hadn’t seen a gap at all, but from my point of view there was a clean cut in the film: no sense of time passing, just one frame and then the next. That’s what anterograde amnesia feels like—the recording stops, even though the behavior continues. But this case didn’t sound like that. I’d have to dig deeper to make sense of it.
Mr. V was not a stereotypical “problem client.” He had a degree in English literature and had served several years in the United States Marine Corps. During his deployment to Iraq, he saw extensive combat. He reported multiple roadside bomb explosions close enough that he may have briefly lost consciousness, though he never sought medical attention at the time. In the Second Battle of Fallujah, he was wounded in street‑to‑street fighting, shot in the arm and leg, and struck by shrapnel while lying prone under machine‑gun fire beside a fellow Marine who was killed. Given that history, it was reasonable for his attorney—and for me—to wonder whether posttraumatic stress or a “trip‑wire” startle response might have played a role in the assault. As the evaluation progressed, however, it became clear that his combat history was part of the background, not the primary cause of what happened in that bedroom.
At the time, I had no reason to think this evaluation would be more interesting than many others on my desk. It turned out to be one of the most instructive cases of my career, and I eventually wrote it up as a case study for a forensic psychology journal. A more detailed, technical version of Mr. V’s case appeared in the Open Access Journal of Forensic Psychology; what follows is a condensed version of that report, rewritten in plain language for non‑specialists, with his informed consent.
Before preparing that article, I spoke with the defendant to make sure he was comfortable with the idea, and I explained that I would disguise his identity and let him review the manuscript before submission. He was pleased to have his experience used that way, but he had one request: he wanted to be referred to as Mr. V—“V for victory,” a nod to his Marine background.
What the records showed that night
The police reports told a clear story. According to his girlfriend, Mr. V had gone to bed as usual after an ordinary evening together. In the early hours of the morning, she awoke to find him gasping and jerking in his sleep, then rolling out of bed and striking his head on a guitar by the nightstand, opening a scalp laceration so that he was bleeding.
She reported that he did not respond to her efforts to wake him and soon began punching the walls and a bureau with enough force to later be diagnosed with a broken hand. Frightened and unsure what to do, she left the room and called for help. The EMTs arrived about fifteen minutes later. One of them entered the bedroom and found Mr. V sitting naked and cross‑legged on the floor, staring ahead and not answering questions. She came closer and gently shook his shoulder to see if he would respond. Without warning, he sprang to his feet and punched her in the face, breaking her nose. She fled the room and reported that he followed her briefly but did not leave the house. By the time additional officers arrived, the residence was surrounded and Mr. V was taken into custody without further incident.
When Mr. V came to my office, I asked him to tell me everything he could remember about what had happened. He said he remembered spending the evening with his girlfriend up until the point they went to bed. His next clear memory was of finding himself outside, some distance from the house, naked and looking up at the sky. He initially thought he was having a dream but eventually realized he was not.
At that point, he noticed he was bleeding from the head. He went back into the house and got dressed, feeling tired and “out of it.” His girlfriend was not there, which puzzled him. When the phone rang, he assumed it was her, but instead he heard a police officer on the line. Mr. V was told to stay where he was and that officers would be arriving shortly. After a brief pause, he was instructed to walk out of the house, which he did, and found himself confronted by a SWAT team. He was arrested and handcuffed. The officers noted that he appeared unwell and took him to the hospital to be evaluated.
Notes from his emergency room treatment indicate that Mr. V presented with intermittent chills, flushing, and fatigue but told doctors that he no longer felt confused or dizzy, as he had immediately upon regaining consciousness that morning. A drug screen was positive for marijuana but negative for other substances, including alcohol. His use of the drug was not considered a significant factor in understanding the assault.
One of the ER physicians reviewed Mr. V’s prior medical records and found a neurological consultation from 2001. At that time, he had been experiencing brief episodes that began with a sensation that something strange was about to happen, followed by a phrase or part of a song running through his head for about 45 seconds, and then a period of marked fatigue. He underwent EEG and MRI testing. The EEG showed abnormal electrical activity, including scattered high‑amplitude signals and brief runs of “sharp waves”—patterns often seen in people with seizure disorders. The MRI revealed an arachnoid cyst in the left temporal fossa, a fluid‑filled pocket near the surface of the brain in the temporal lobe. The neurologist suspected that these episodes represented simple or complex partial seizures and recommended further evaluation, but Mr. V did not return for follow‑up, most likely because he was concerned that a seizure diagnosis would interfere with driving and with his plans to join the military.
However, based on her review of his actions, presentation, and prior history, the attending physician provisionally diagnosed temporal‑lobe epilepsy and ordered a follow‑up ambulatory EEG. Temporal‑lobe epilepsy is a form of seizure disorder in which the abnormal electrical activity begins in one of the temporal lobes, areas involved in memory and emotion; people with this condition may have brief episodes of altered awareness and can be confused or agitated in the period immediately after a seizure. The results of the ambulatory EEG confirmed the diagnosis, and Mr. V was started on anticonvulsant medication.
Testing and what it ruled out
After taking Mr. V’s history, I began the testing part of the assessment. This included a mental-status examination, a more detailed clinical interview, a review of his records, and administration of the Personality Assessment Inventory (PAI), a comprehensive questionnaire used to detect problems such as depression, anxiety, anger-control difficulties, or mania, as well as a way to check whether someone might be exaggerating or downplaying their symptoms. I also administered the MicroCog, a computerized neuropsychological screening instrument that provides a quick look at areas such as attention and memory. Mr. V’s presentation during the mental‑status examination was largely unremarkable, apart from some fidgeting and restlessness suggestive of possible mild residual attention‑deficit/hyperactivity disorder.
Mr. V’s PAI profile was valid and showed no clinically significant elevations that would suggest major psychological disorders. There were some signs of trauma-related symptoms, but no evidence of full post-traumatic stress disorder, which was consistent with his own report. His MicroCog results were somewhat unusual in that he scored in the low‑average range on measures of short‑term and immediate memory, which was surprising given his recent graduation from college. However, there was no indication that these findings reflected a level of neuropsychological impairment that was significantly affecting his day‑to‑day functioning.
The psychological testing largely ruled out the usual explanations for a sudden assault. There was no major mood or psychotic disorder, no personality profile marked by chronic aggression, and no severe cognitive impairment that might account for grossly disorganized behavior. His combat history and some trauma‑related symptoms were clinically relevant, but there was no evidence of full post‑traumatic stress disorder, and nothing in his presentation suggested a classic “hair‑trigger” rage pattern. There was no indication of intoxication beyond marijuana, and no sign of planning, motive, or attempts at concealment. Taken together, that left me with a troubling gap: a serious, apparently senseless assault with no clear psychological explanation.
His history and the seizure diagnosis
With no obvious psychological explanation, I had to look harder at the medical side of the case. The emergency room notes stated that Mr. V presented with intermittent chills, flushing, and fatigue but told doctors that he no longer felt confused or dizzy, as he had immediately upon regaining consciousness that morning. A drug screen was positive for marijuana but negative for other substances, including alcohol. His use of the drug was not considered a significant factor in understanding the assault.
One of the ER physicians reviewed Mr. V’s prior medical records and found a neurological consultation from 2001. At that time, he had been experiencing brief episodes that began with a vague sense that something strange was about to happen, followed by a phrase or part of a song running through his head for about 45 seconds, and then a period of marked fatigue. He underwent EEG and MRI testing. The EEG showed abnormal electrical activity, including scattered high‑amplitude signals and brief runs of “sharp” waves—patterns often seen in people with seizure disorders. The MRI revealed an arachnoid cyst in the left temporal fossa, a fluid‑filled pocket near the surface of the brain in the temporal lobe. The neurologist suspected that these episodes represented simple or complex partial seizures and recommended further evaluation, but Mr. V did not return for follow‑up, most likely because he was concerned that a seizure diagnosis would interfere with driving and with his plans to join the military.
Based on her review of his actions, presentation, and prior history, the attending physician provisionally diagnosed temporal‑lobe epilepsy and ordered a follow‑up ambulatory EEG. Temporal‑lobe epilepsy is a form of seizure disorder in which the abnormal electrical activity begins in one of the temporal lobes, areas involved in memory and emotion; people with this condition may have brief episodes of altered awareness and can be confused or agitated in the period immediately after a seizure. The results of the ambulatory EEG confirmed the diagnosis, and Mr. V was started on anticonvulsant medication. For a case like this, that earlier history suddenly mattered a great deal.
The familiar explanations for sudden violence did not account for what happened in that bedroom. Most evaluators do not start with a seizure-related explanation when they encounter an assault like this, and neither did I. In this case, though, the accumulating evidence kept nudging me away from those familiar possibilities and toward a brief postictal episode related to his temporal‑lobe epilepsy.
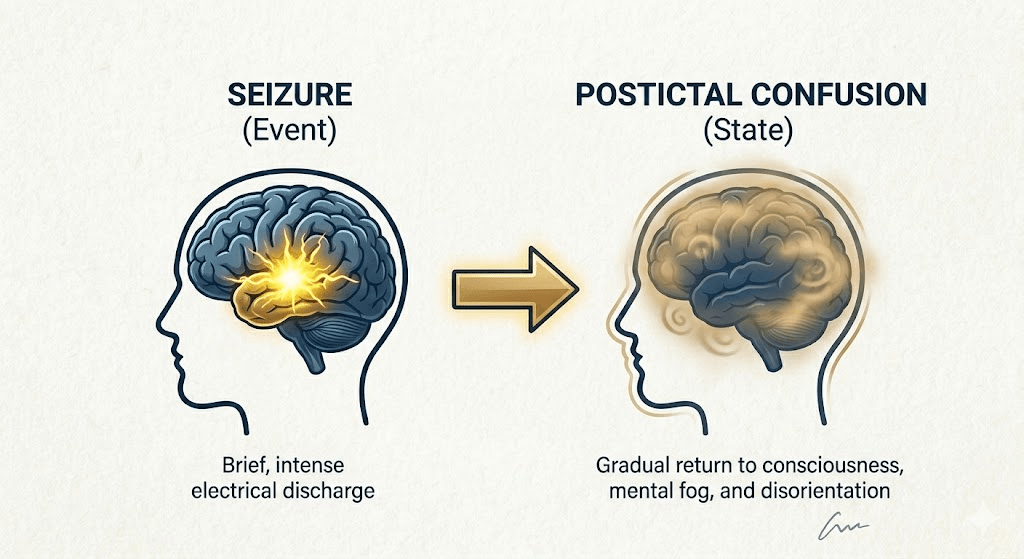
To understand what Mr. V did in that bedroom, we need a couple more pieces of information from neurology. Neurologists use the word “postictal” for the period right after a seizure, when the brain is still recovering. During this time, people can be confused, disoriented, or agitated and may not think or respond normally.
“Epileptic automatism” refers to actions that happen during or just after a seizure when a person’s awareness is severely impaired. From the outside, the behavior can look purposeful—walking, talking, even striking out—but from the inside, the person is not fully conscious of what they are doing and often has no memory of it afterward.
I didn’t start out thinking the incident was a seizure case. Like many forensic psychologists, I was trained to consider trauma, substance use, personality factors, and major mental illness when trying to understand sudden violence. In this case, those lines of inquiry did not account for what had happened.
What brought seizures to mind was an experience I’d had years earlier in graduate school, during a guest lecture by a noted neurologist on seizure disorders. The neurologist began describing complex partial seizures in abstract terms, and then, without warning, shifted into a demonstration: he stopped speaking, moved around the room in an odd, searching manner, and behaved as if he were looking for something he could not find. Only afterward did he explain that the demonstration was how some patients appear during a seizure—awake and moving, but not fully aware or in control. That image stayed with me.
I summarized these findings and opinions in a report for the court, and the defense attorney submitted it. The prosecutor requested a hearing so that I could explain the seizure‑related conclusions in more detail; there was no reason to expect him to be an expert on epilepsy or postictal states. After hearing the testimony and asking questions, both the prosecutor and the judge indicated that the seizure explanation made more sense of the facts than any competing theory they had considered. They had been struggling to understand why Mr. V—a generally pleasant, law‑abiding man and decorated combat veteran—would suddenly punch an EMT who was trying to help him; the postictal automatism framework fit the available evidence. Rather than pursue a contested insanity/NGRI route, the prosecutor moved to dismiss the assault charge outright, accomplishing the same practical goal—no conviction—while avoiding additional time, expense, and strain on everyone involved.
Postictal automatism and responsibility
Cases like Mr. V’s are rare, but they illustrate why careful history taking, record review, and collaboration with neurologists matter in forensic work. Most people with epilepsy are never violent, and most violence has nothing to do with seizures. But when an apparently senseless act occurs in the immediate aftermath of a documented seizure, especially in someone with a prior seizure history or neurological injury, it is worth exploring not just what the person did, but what their brain was capable of at the time. For me, the lesson in this case was simple but uncomfortable: if we stop at the first plausible story—trauma, intoxication, bad character—we can miss the real explanation and risk doing serious harm. Careful history-taking, collaboration with medical colleagues, and a willingness to revise our theories are not just clinical virtues; in cases like this, they can be the difference between a criminal record and justice.
In future posts, I’ll look more closely at how courts handle cases where the line between mental illness, neurological disorder, and criminal responsibility is less clear.
If you want to read the original article, follow this link to the Open Access Journal of Forensic Psychology: https://a091bcda-ef2e-423a-8e26-23fa0ffe04ed.filesusr.com/ugd/166e3f_28f9b9d82c874d2a9df9006d8a3b8804.pdf
Discover more from Samurai Shrink (formally Wandering Shrink)
Subscribe to get the latest posts sent to your email.
